Cervical collars and spinal cord injury protection
June 14, 2024
It’s not a black and white choice of collar or not, good or bad, routine or never.
In the setting of an actual or probable cervical spine injury, providing stability control is widely accepted as better than providing no stabilization at all. It is then an issue of how best to provide that stability control.
The choice is dynamic, not “set and forget”. Two things are important in making one’s choice:
- Being able to justify the choice based on a sound assessment of the evidence and how it applies to a given patient (Evidence based practice)
- Keeping track of outcomes over time in order to confirm or refute one’s choice, or adapt as the context or evidence evolves (Quality improvement)
Themes that seem to emerge when reading cervical spine injury and collar literature:
- Overall in the trauma population, cervical spine injury (bone injury) incidence is low (2-4%) and cervical spinal cord injury is lower again. This incidence increases with age and mechanism and is strongly associated with the incidence of TBI.
- CSI is a higher likelihood in the unconscious or obtunded patient rather than the alert, appropriately responsive patient
- CSI typically occurs alongside other traumatic injuries such as chest, abdomen and head.
- About 1 in 8 patients with CSI goes for surgery with the remainder managed either with a temporary orthotic collar (eg. Aspen, Miami J, other) – the majority – or no intervention at all (5%)
- While the risk of secondary cervical spinal cord injury from minimal movements of the neck or non-application of a semirigid collar are probably extremely low and the risk of resultant permanent neurological deficit is even lower, neither are zero.
- The majority of neurological deterioration following an actual spinal cord injury is due to local swelling rather than minimal movements of the neck. As the local swelling settles, there is usually improvement in neurology.
- The majority of epidemiological reduction in complete quadriplegia and increase in life expectancy appears to be more attributable to safer vehicle engineering, better legislation and education (prevention) rather than emergency and trauma clinical and procedural care developments (cure).
- The quality of evidence to guide the choice of cervical spine stabilization strategy prior to definitive intervention is largely low grade. This is not indicative of poor research, rather it is the result of it being a difficult thing to study in a relatively low incidence injury, with trials restricted to surrogate measures of efficacy and outcome; eg cadaver studies, healthy volunteer motion studies.
The problem
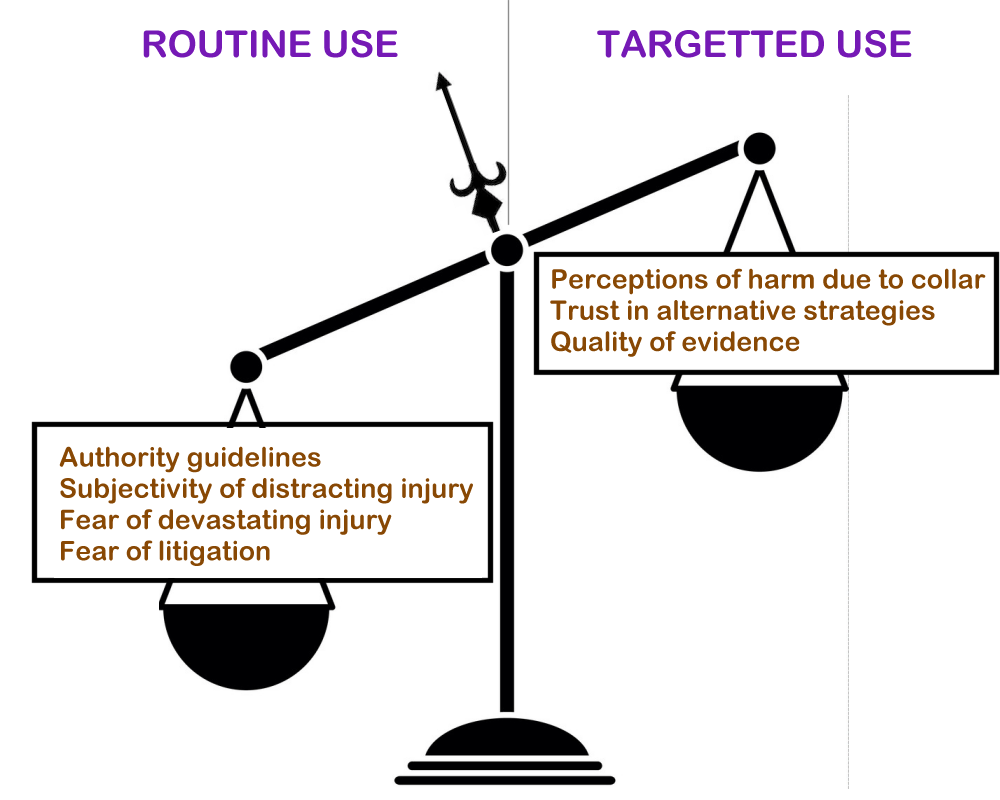
Authority recommended spinal immobilization of all trauma patients with a known or suspected CSI or SCI + fear of a devastating patient outcome +/- fear of medicolegal repercussions balanced against a perception of relatively little harm from applying a semi-rigid collar -> routine use of semirigid collars just to cover the possibility +/- the often subjective nature of assessing the impact of a distracting injury.
Collar options
Rigid – Generally applied once in hospital once an injury has been confirmed or cannot be excluded despite appropriate work up. Typically fitted by a trained practitioner; e.g. doctor, physiotherapist, nurse practitioner.
Semi-rigid – The stalwart piece of prehospital and emergency department equipment.
- Requires training to be able to use properly.
- Typically seen strapped around the thigh of a responding medic and for a long time features prominently in trauma response procedures (ATLS, EMST, AANS/CNS Joint Guidelines, etc), right up there with securing an open Airway (A + C-spine, B, C, D).
- Available in fixed-size and adjustable versions.
- Over the past ten to fifteen years there have been increasing concerns about harms attributed to semi-rigid collars such as pressure wounds, impaired cerebral venous drainage and subsequent secondary brain injury, aspiration risk as these patients are often left lying on their backs until their spine has been cleared, interference with Rapid Sequence Intubation which requires the collar to be removed anyway.
Soft collars – Previously dismissed as no more than foam neck warmers, the use of soft collars has undergone a resurgence since the early to mid twenty-teens when concerns over the unproven efficacy and potential for harm of the semi-rigid collars started to take hold. It is acknowledged that soft collars provide almost no neck stabilisation and instead act as an alert to clinicians that the cervical spine has not yet been cleared of injury. A sticker on the patient’s chest or forehead would do the same job.
Other options – The OTEC AER Collar: Marketed as being at least as effective as a semi-rigid collar but with the safety profile of a soft collar. The AER Collar is a shaped, pneumatic collar that is placed around the patient’s neck and then inflated. The design is appealing for a number of reasons:
- It folds up to a much smaller size than any other form of collar when not in use
- It is easy to position around the neck of a patient regardless of where they are; eg. on a stretcher, seated in a car (particularly relevant for motorsport where seat and cockpit design often hamper attempts to place a more rigid type of collar)
- Once inflated, it seems as least as supportive as a semi-rigid collar and certainly more so than a soft, foam collar. The manufacturer has published comparative degrees of motion for the AER Collar here ->
- Once inflated it seems at least initially to distribute its pressure on the chin, jaw line, occiput and shoulder fairly evenly, which is part of its marketed claim of reduced risk of pressure wound development.
Having given a couple of AER collars to paramedics and doctors to play with at several motorsport events between February and June, including circuit and rally-raid events, these features were quickly identified by the clinicians as positive qualities of the collar. There were however some limitations:
- The limitation of excess movement of the person’s neck seemed a lot less contained than with a semi-rigid collar. Movement was limited if the person kept relatively still, as they would likely do if they had pain or were complying with the clinician’s directions. However, excessive movement could be achieved with relatively little effort in all directions. Whether or not this would happen in real use has not been formally tested.
- While the AER Collar was initially more comfortable than a semi-rigid collar, most clinicians noted some tendency to discomfort from pressure on their chin and jaw line and a little later, on the trapezius muscle region of the shoulder. Whether or not this might eventually result in a pressure wound was not formally tested.
- The pneumatic mechanism for firming up the collar allows for a small storage volume and ease of fitment. However, there were concerns from clinicians that there may be an associated risk of imparting a distracting force on a bone or ligamentous injury during or with excessive inflation, resulting in a potential for secondary spinal cord injury. Perhaps the inclusion of a “optimum inflation gauge”, similar to the pilot balloon of an ET tube, might help here.
- Some concerns were raised regarding the use of an air-filled device during patient transport. Air leak and resulting deflation would negate any potential benefits of the collar and though it can be topped up as needed, this requires constant monitoring of the collar during transport. Overinflation was also a concern for aeromedical transport. This is less likely to be a significant problem as fixed wing transport is often a pressurised cabin and rotary wing transport generally does not occur at an altitude that results in large pressure-volume changes.

Again, the conversation should not be diverted to a competition of what collar is the best, but instead should keep a focus on whether and how best to use a collar, if at all.
We know from several studies, the most recent of which was the EXIT Project, that there is less movement and discomfort when a person self extricates from their vehicle than when they are eased out by rescuers, whether or not a collar is applied. The EXIT Project also demonstrates that several factors influence the risk profile of a given patient, such as age, duration of entrapment, impaired consciousness. A collar may be helpful when the person is not fully alert, has a significantly distracting injury or where there are not enough rescuers present to ensure stability. The key points in any of these situations include that the application of a collar need not be a routine manoeuvre and its deployment should be tailored to the specific circumstance of that patient and once the patient is secured in an appropriate position on a suitable stretcher, the collar should be removed unless there is a very clear reason to keep it in place.
So, it is more about making a judgement on what the patient needs, how best to achieve the desired outcome for that patient and what are the acceptable and unacceptable risks of each choice; which is essentially what we are supposed to do as professional clinicians.
References
- Prehospital use of cervical collars in trauma patients: a critical review. Sundstrøm T, Asbjørnsen H, Habiba S, Sunde GA, Wester K. J Neurotrauma. 2014 Mar 15;31(6):531-40. doi: 10.1089/neu.2013.3094. Epub 2013 Nov 6.
- Prehospital Cervical Spinal Immobilization After Trauma. Nicholas, Theodore; Hadley, Mark N; Aarabi, Bizhan; Dhall, Sanjay S; Gelb, Daniel E; et al. Neurosurgery; Philadelphia Vol. 72, (3), (Mar 2013): 22-34.
- Transportation of Patients With Acute Traumatic Cervical Spine Injuries. Nicholas, Theodore; Aarabi, Bizhan; Dhall, Sanjay S; Gelb, Daniel E; Hurlbert, R John; et al. Neurosurgery; Philadelphia Vol. 72, (3), (Mar 2013): 35-39.
- Value of a rigid collar: in need of more research and better devices
- Smyth, Mike; Cooke, Matthew W. Emergency Medicine Journal Vol. 30, (6), Jun 2013.
- Cervical collars: probably useless; definitely cause harm! Plumb, James O M; Morris, Craig G. The Journal of emergency medicine Vol. 44, (1), (January 2013): e143
- Cervical spine motion during extrication. Engsberg, Jack R; Standeven, John W; Shurtleff, Timothy L; Eggars, Jessica L; Shafer, Jeffery S; et al. The Journal of emergency medicine Vol. 44, (1), (January 2013): 122-127
- A Delphi study of rescue and clinical subject matter experts on the extrication of patients following a motor vehicle collision. Nutbeam, T., Fenwick, R., Smith, J.E. et al. Scand J Trauma Resusc Emerg Med 30, 41 (2022). https://doi.org/10.1186/s13049-022-01029-x
- Biomechanical analysis of spinal immobilisation during prehospital extrication: a proof of concept study. Dixon M, O’Halloran J, Cummins NM. Emerg Med J. 2014;31:745–9.
- Confirmation of suboptimal protocols in spinal immobilisation? Dixon M, O’Halloran J, Hannigan A, Keenan S, Cummins NM. Emerg Med J. 2015;32:939–45.
- Use of foam collars for cervical spine immobilisation. Agency for Clinical Innovation. https://aci.health.nsw.gov.au/__data/assets/pdf_file/0009/450882/ACI-Foam-collars-cervical-spine-immobilisation-initial-management.pdf (A downloadable PDF document)
- The OTEC AER Collar (Website). https://www.otecdesign.com/product
Disclosures
The author of this review was provided with two OTEC AER Collars to trial by the manufacturer.
Posted by Matthew Mac Partlin. Posted In : Clinical topics